The gut microbiome
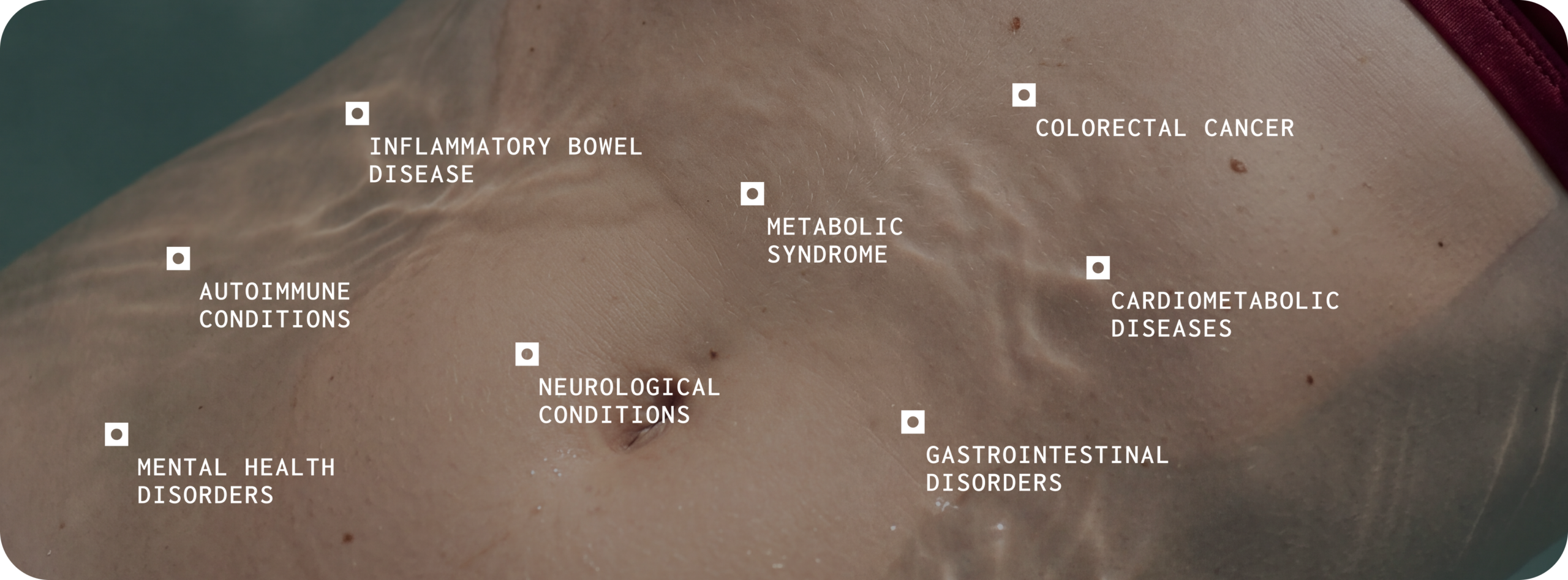
The human gut harbours trillions of microorganisms whose collective genome — the microbiome — encodes metabolic capabilities far exceeding those of the human genome alone.1 Over the past two decades, large-scale sequencing studies have demonstrated that the composition and function of this microbial community are associated with a wide range of health outcomes.2,3 Disruption of a healthy gut microbiome, often called dysbiosis, has been linked to gastrointestinal disorders, autoimmune conditions, cardiometabolic diseases, and neurological conditions.4
The Clinical Question:
The clinical question is straightforward: can we measure a patient’s gut microbiome accurately enough and interpret the results rigorously enough, to inform care?
Testing has evolved. Not all tests have.
Many gut health tests available today rely on older methods — culture-based assays, quantitative PCR (qPCR), or 16S ribosomal RNA (rRNA) gene sequencing that provide only a partial view of the microbiome5,6.
These approaches can be good in specific circumstances (e.g. identification of pathogens), but have well-documented limitations in their ability to identify microbes at species level, coverage of the entire microbiome, and the ability to assess microbial function.5,6
A step change in capability
The emergence of shotgun metagenomics — sequencing all DNA in a sample rather than a single gene has fundamentally changed what is possible, enabling species and even strain-level identification alongside functional pathway analysis.7
Technology alone isn’t enough
The quality of the reference data results are compared against, and the rigour of the evidence framework used to interpret them, determine whether that technology translates into something a practitioner can actually rely on. This paper documents how Microba has built to that standard at every layer — because the quality of the science behind a test determines the reliability of the result.
Accurate gut testing starts with the fundamentals
MEASUREMENT TECHNOLOGY
The sequencing method used to capture the microbial community and its resolution, coverage, and accuracy
REFERENCE DATA QUALITY
The reference cohort against which results are compared and whether it eliminates bias
SCIENTIFIC FRAMEWORK
The evidence framework that turns microbiome data into something clinically useful
Microba Microbiome Explorer
The quality of a result comes from everything behind it
Microba Microbiome Explorer combines accredited gastrointestinal diagnostics with high-resolution shotgun metagenomic microbiome profiling. Pathogen detection and gastrointestinal markers are CE-certified and run within an ISO 15189 NATA-accredited medical laboratory. This deep dive covers the complete scientific and technological foundation — from how a sample is preserved, through to the clinical insights a practitioner reads in the report.
100,000+
Metagenomes processed. Operational track record
28,000+
Species assessed Species-level profiling
99%
Precision rate Virtually zero false positives
19,000+%
Consented profiles Internal validation dataset
Validated sample preservation
protects the accuracy of every result
The moment a sample is collected, the clock starts. Microbial composition shifts fast if preservation isn’t handled correctly — and most collection methods weren’t designed with that in mind.
Microba’s FLOQSwab-ADT was benchmarked head-to-head against the most widely used alternatives.⁸
It demonstrated the strongest performance in the evaluation. Practitioners can be confident the sample that leaves the patient’s home is the sample that gets analysed. No degradation. No compromise.
Best reproducibility
Highest technical (between-replicate) reproducibility and compositional stability relative to flash-frozen controls in a peer-reviewed evaluation
Climate resilient
Stable across −20°C, room temperature, and 50°C for four weeks — suitable for postal collection Australia- wide
Practitioners can be confident that the microbial profile generated from a swab collected at home closely reflects the true composition of the patient’s sample at the time of collection.
001
Patient collects
at home
002
FLOQSwab-ADT
preserves sample
003
Postal delivery in
any climate
004
Microba lab receives
intact sample
Did you know?
Microbial markers are scientifically curated using a rigorous three-tier evidence framework, and results are compared against a carefully defined healthy reference group of more than 450 individuals.
Over 100,000 metagenomes processed in an accredited laboratory.
Accreditation sets the floor. What happens inside the laboratory is what raises it. Microba operates an ISO 15189 NATA-accredited medical testing laboratory, the internationally recognised standard for medical laboratories — running the latest DNA sequencing technology at a high level of automation from sample receipt through to data generation.
Every sample is monitored by an automated quality control pipeline. Anything that falls outside predefined quality thresholds gets flagged before it goes further. More than 100,000 metagenomes processed – an established operational track record.
High quality doesn’t stop at the bench
The software systems used to analyse and interpret metagenomic data are developed under an ISO 13485 quality management system for software as a medical device.
Most providers stop at laboratory accreditation. Dual accreditation — ISO 15189 for laboratory processes and ISO 13485 for the bioinformatic pipeline, means the same rigour applies to how data is analysed, not just how it’s collected
ISO 15189
Internationally recognised standard for medical laboratory processes —
covering sample receipt, sequencing, and data generation
ISO 13485
Quality management system for software as a medical device —
covering the bioinformatic analysis and interpretation pipeline
Shotgun metagenomics identifies species that other methods miss entirely
Shotgun metagenomics sequences all DNA extracted from a faecal sample – not a single gene, not a predefined panel. The result is a comprehensive, relatively unbiased view of the entire microbial community at species level (not genus level).⁷
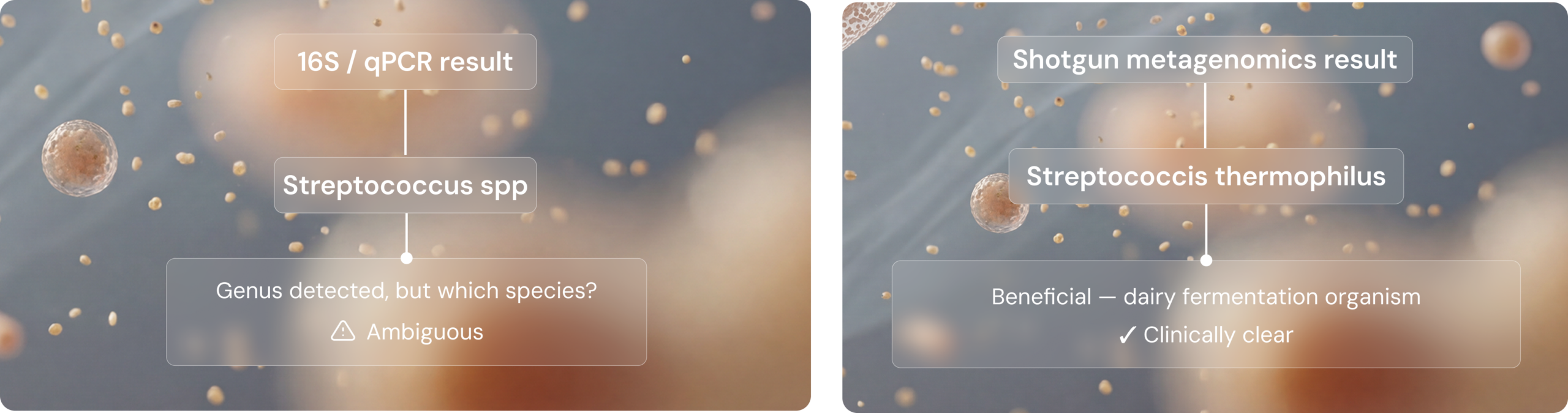
That distinction matters more than it sounds. Different species within the same genus can have very different roles in health. Without species-level resolution, you’re working with an incomplete picture. Take the genus Streptococcus. Streptococcus thermophilus is considered beneficial and widely used in dairy fermentation. Streptococcus anginosus is an opportunistic pathogen associated with atherosclerosis and systemic lupus. Same genus. Completely different clinical implications.
A test that can only tell you ‘Streptococcus’ is present isn’t giving you enough to act on.
The Streptococcus example
Comparison of microbiome testing methodologies
632 species vs 57
In a direct comparison, shotgun metagenomics identified 632 species in a sample where 16S rRNA gene sequencing detected only 5714 — an order-of-magnitude difference in resolution that directly affects clinical utility.

Species tell you who’s present, function tells you what they’re doing
Identifying what’s in the microbiome is the starting point, not the finish line. Shotgun metagenomics goes further, identifying not only the species, but also the presence of key health-associated metabolic genes and pathways across the entire microbial community. That means assessing functional capacity – what that community is capable of doing. Can this community produce butyrate? Is there a high relative abundance of species that can consume mucin? These are the questions that move a result from interesting to actionable. Other methods such as 16S rRNA sequencing and metabolite measurements can’t get you there.
18.96%
Butyrate-producing capacity detected. Even when other tests reported none.
Assessing functional potential provides clinically relevant context
Other tests may report faecal concentrations of metabolites such as butyrate and stop there.
However, faecal butyrate concentration alone does not distinguish between microbial production, host absorption, microbial utilisation, and transit-related effects. Because faecal short-chain fatty acid concentrations do not directly measure total colonic production, low faecal butyrate does not necessarily indicate reduced butyrate-producing capacity. Other tests may report faecal concentrations of metabolites such as butyrate and stop there.
A microbiome may have butyrate-associated pathways yet show low faecal butyrate due to current output being constrained by dietary substrates, colonic conditions such as pH, microbial cross-feeding, transit times, or efficient host uptake.
Clinically, that distinction matters. It shifts interpretation from whether butyrate is low in stool (a finding that may have several possible explanations) to whether the microbiome retains the functional potential to produce butyrate under the right dietary and ecological conditions. Compared with faecal metabolite testing, 16S rRNA sequencing, or targeted qPCR, shotgun metagenomics provides a broader, community-wide view of functional potential.
The Microba Community Profiler achieves 99% precision — peer-reviewed and benchmarked
Generating sequence data is only the first step. What you do with it is where most tools fall short. The accuracy
of a microbiome profile depends entirely on the bioinformatic tools used to classify millions of short DNA sequences and not all classifiers are built to the same standard.
The Microba Community Profiler (MCP) is a proprietary whole-genome alignment tool purpose-built to
produce species-level community profiles with the highest possible accuracy. Its performance has been
formally benchmarked in a peer-reviewed study in Frontiers in Microbiology — evaluated against nine widely
used academic classifiers across 140 simulated microbial communities of varying complexity. The benchmarking results highlight the difference.
The Microba Community Profiler (MCP) is a proprietary whole-genome alignment tool purpose-built to
produce species-level community profiles with the highest possible accuracy. Its performance has been
formally benchmarked in a peer-reviewed study in Frontiers in Microbiology — evaluated against nine widely
used academic classifiers across 140 simulated microbial communities of varying complexity. The numbers tell
the rest of the story.

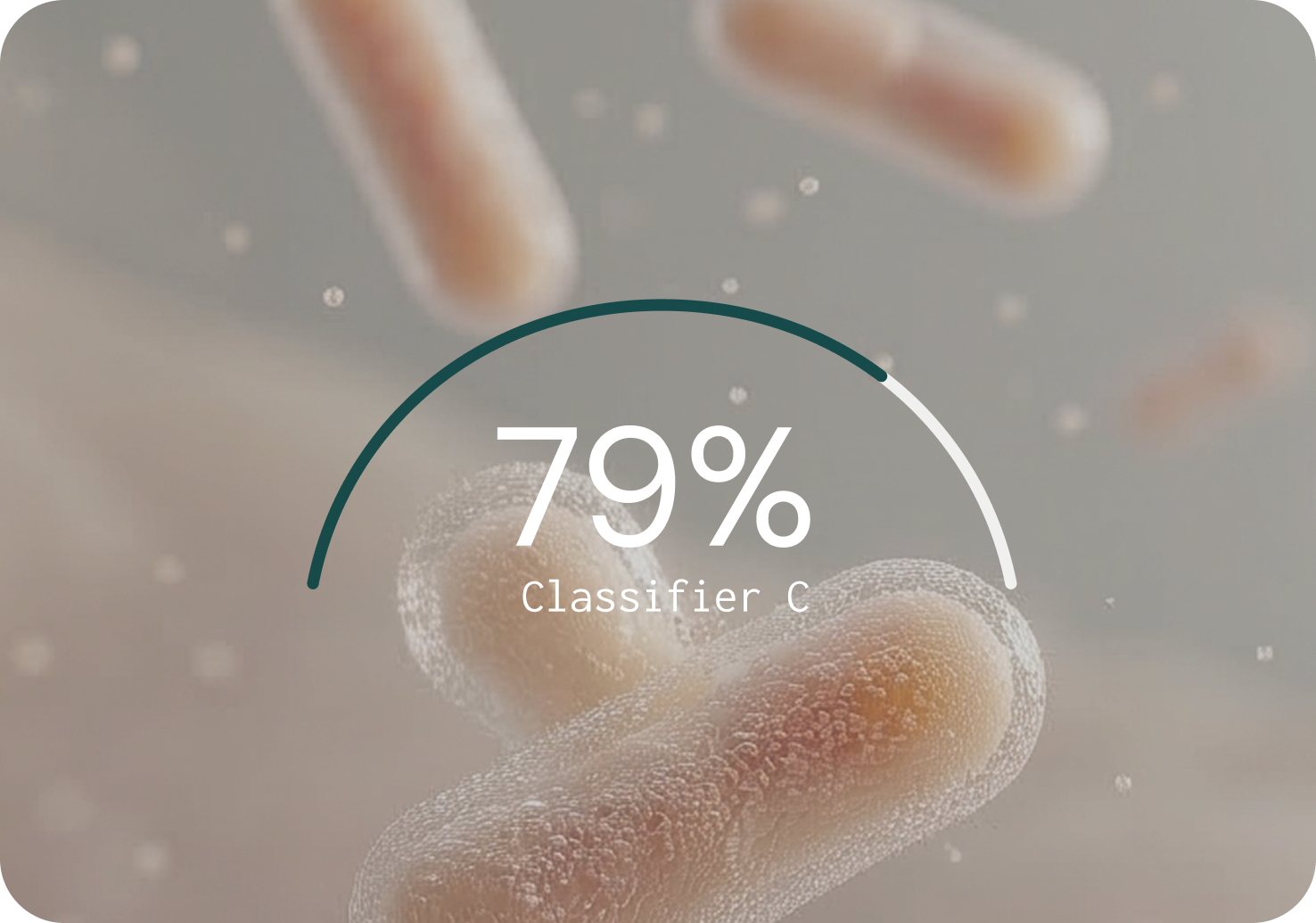
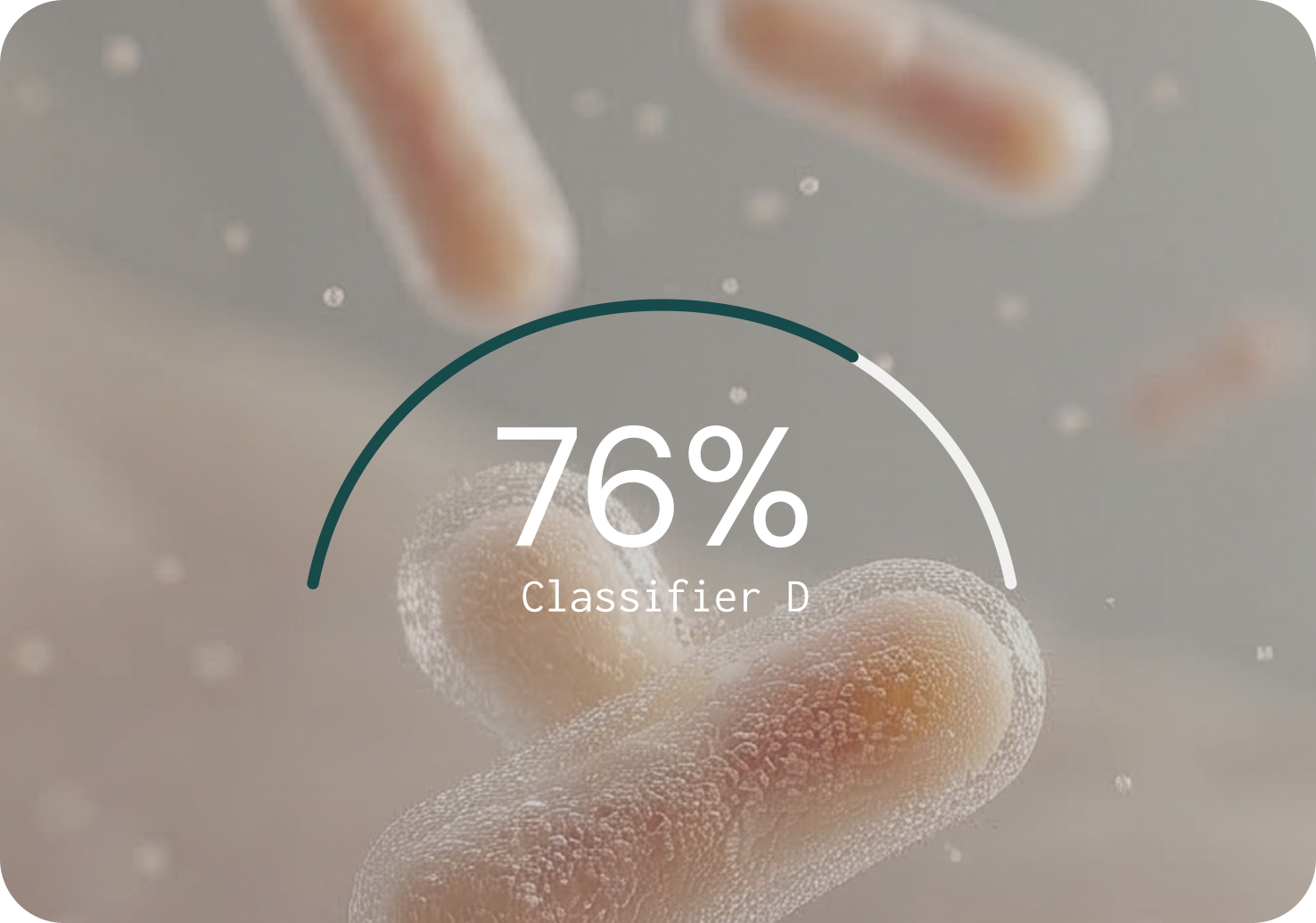
Against nine widely used classifiers, MCP had the strongest overall performance
Three integrated layers translate microbial presence into clinical meaning
No single marker tells the whole story. Microba Microbiome Explorer integrates three layers of information to connect what’s present in the microbiome with measurable clinical markers of gut function and inflammation.
PATHOGEN DETECTION
A panel of 13 common bacterial pathogens and five parasites detected via CE-certified multiplex PCR assays.
HUMAN STOOL MARKERS
Six GI health markers including calprotectin, lactoferrin, faecal occult blood, secretory IgA, pancreatic elastase, and zonulin — assessed using CE-certified immunohistochemistry assays. Faecal pH is also measured as an investigative marker for research use only.
MICROBIOME PROFILING
Species-level profiling of 28,000+ species including microbial diversity, richness, and 16 health-associated functional markers — such as butyrate production, trimethylamine, hexa-acylated lipopolysaccharides, mucin degradation, and oxalate consumption. For research use only.
Separately, each layer is informative. Together they deliver something no single method can. By combining diagnostic gastrointestinal markers with microbiome profiling, the test moves beyond simple species detection to provide a functional picture of gut health, linking what is present in the microbiome with measurable clinical markers of gut function and inflammation.
Reported markers are clinically relevant and evidence-backed
Not every microbial signal is clinically meaningful. To ensure that the microbiome markers reported in the test are supported by robust evidence, Microba applies a rigorous three-tier scientific curation framework. Only markers that satisfy all three tiers (with limited, clearly disclosed exceptions) are included in the report.* Every marker a practitioner sees has cleared a high evidence bar, nothing is included on association alone.
*A small number of markers are included with clearly disclosed exceptions — acetate and intestinal inflammation, beta-glucuronidase and impaired detoxification (both mechanism only), and Emerging Markers. Where exceptions exist, they are explicitly flagged in the report.
MICROBIAL SIGNALS
Thousands of possible associations from the literature
REPRODUCIBLE HUMAN ASSOCIATIONS
At least two peer-reviewed human studies must show a direct and/or indirect link between the marker and the health outcome.
SCIENTIFIC VALIDATION
Only markers validated in Microba’s 19,000+ profile dataset (FDR < 0.05)
Tier 1 Plausible mechanism of action
There must be in-vitro or in-vivo data demonstrating why the microbial marker is biologically connected to the relevant health category. Example: the link between mucin-degrading species and intestinal inflammation is supported by mechanistic studies showing that depletion of the mucus barrier increases microbial proximity to the epithelium, driving immune activation.10-13
Tier 2 Reproducible human associations
At least two peer-reviewed human studies must show a direct and/or indirect link between the marker and the health outcome. Example: Direct evidence: published association between the marker and a clinical measure (for example, faecal calprotectin).
Indirect evidence: an association between the marker and a relevant clinical condition, or between plasma levels of the microbial product and a clinical measure.
Tier 3 Significant associations in Microba’s dataset
The marker must show a statistically significant association in Microba’s own database of 19,000+ consented patient profiles, controlled for age, sex, BMI, and bowel habits. This validation step ensures markers are not only literature-supported but also reproducible within a large, independent cohort processed through Microba’s laboratory and bioinformatics pipeline. Example: This internal validation step ensures that markers are not only supported by published literature but are also reproducible in a large, independent cohort processed through Microba’s own laboratory and analysis pipeline.
The reference group determines the quality of every result
INCLUSION CRITERIA
No major medical conditions
No or minimal GI symptoms· Mild or lower stress, anxiety, and depression
BMI below 30 Daily fruit and vegetable intake
Low to moderate alcohol consumption
The report tells you what’s there, evidence-graded actions tell you what to do about it.
Generating accurate microbiome data is necessary but not sufficient. For gut health testing to be clinically useful, the data must be translated into interpretable insights that healthcare practitioners can act upon. In Microba’s Microbiome Explorer, microbial markers and gastrointestinal markers are organised into health categories that correspond to recognisable clinical concepts applicable, links to the relevant diagnostic GI markers for clinical correlation. Each health category provides a clear interpretation of whether the patient’s results fall within or outside the healthy reference range, and, where applicable, links to the relevant diagnostic GI markers for clinical correlation.
When a marker is identified as out of range, the report provides evidence-graded possible actions.
Microba’s science team has undertaken a rigorous review of the available scientific evidence for different dietary, supplement, or lifestyle interventions to modulate microbial functions and graded these using the NHMRC evidence grading framework. Each listed action is accompanied by the evidence grade and hyperlinks to the references that informed the grade.
Mucin degradation and intestinal
inflammation
The proportion of mucin-degrading species in the microbiome is one of the markers assessed in the test. The mechanistic basis for this marker is well established: when dietary fibre is insufficient, mucin- degrading microbes can consume the protective mucus layer lining the gut, increasing microbial contact with the intestinal epithelium and triggering immune activation. A large cross-sectional study of more than 1,000 individuals found a significant positive association between mucin-degrading pathway abundance and faecal calprotectin (a clinical marker of intestinal inflammation).14 Elevated mucin degrading pathways have also been observed in colorectal cancer cohorts.15,16 In Microba’s own dataset, the relative abundance of mucin-degrading species is significantly increased in several health conditions related to intestinal inflammation compared to healthy controls, after controlling for confounders.
Built for clinical confidence
This layered approach — mechanistic plausibility, published human evidence, and internal validation, gives practitioners a clear rationale for each marker and a basis for evidence-informed clinical conversations with patients. Microba Microbiome Explorer is exclusively offered through healthcare professionals. This distribution model ensures that results are interpreted accurately, responsibly, and in the best interests of patient care.
This is what sets Microba’s approach apart
The gut health testing market includes a range of product built on different technologies, evidence standards, and quality systems. Several features distinguish Microba’s approach from legacy and competing tests.
not 16S or qPCR
benchmarked bioinformatics
evidence curation
reference group
Science, evidence, and quality integrated to deliver what no legacy test can
Microba’s Microbiome Explorer represents a considered integration of advanced metagenomic science, rigorous evidence curation, and accredited laboratory quality. By combining CE-certified gastrointestinal measures with high-resolution microbiome profiling, the test provides healthcare practitioners with a comprehensive view of gut health that goes well beyond what legacy testing methods can offer. Every layer of the technology stack — from validated sample preservation and automated laboratory processing, through to the peer-reviewed MCP — has been designed to maximise accuracy and minimise the risk of misleading results. The three-tier marker curation framework ensures that only microbial markers with robust supporting evidence are included, and results are compared against a carefully curated healthy reference group.
Microba commitment
Microba is committed to translating advances in microbiome science into testing that practitioners can trust. Every layer of the Microbiome Explorer, from sample preservation through to clinical insights, has been built to the highest scientific and quality standards, and that commitment extends to how
the science evolves.
As new evidence emerges, markers are refined, the reference group expanded, and validation studies continued, so the test remains at the leading edge
of what microbiome science can reliably deliver for practitioners and their patients.
Sample
Collection
Validated FLOQSwab–ADT
Climate-resilient postal
collection
Lab + Data
Generation
ISO 15189 accredited lab
100,000+ metagenomes
Automated QC pipeline
Core
Analysis
Shotgun metagenomics
Microba Community Profiler
(99% precision)
Interpretation
Layer
Three-tier evidence curation
450+ healthy reference group
NHMRC-graded actions
Transparency about limitations is essential for responsible clinical use
it measures the relative proportions of different species rather than their absolute quantities. This is an inherent characteristic of current sequencing technology and means that changes in the abundance of one organism can influence the apparent abundance of others. On average, Microba will be able to assign a species ID to 82.4% of sequencing reads. Microba continues to expand the database with newly identified species and strains, and ongoing updates to the reference database aim to increase the proportion of sequencing reads assigned a species ID and lower detection limits further. The marker curation framework is also a living process: as new evidence emerges, markers may be added, refined, or retired. Future directions include further validation studies, expansion of the healthy reference group to include additional populations, and continued development of evidence-graded suggested actions informed by the latest intervention research.
.*The microbiome component of Microba Microbiome Explorer is for research use only and is not a diagnostic tool. Microbiome results should be interpreted by qualified healthcare practitioners in the context of a patient’s clinical history, symptoms, and other diagnostic findings.
- Lynch, S. V. & Pedersen, O. The human intestinal microbiome in health and disease. N. Engl. J. Med. 375, 2369–2379 (2016). https://doi.org/10.1056/NEJMra1600266
- Gilbert, J. A., Blaser, M. J., Caporaso, J. G., Jansson, J. K., Lynch, S. V. & Knight, R. Current understanding of the human microbiome. Nat. Med. 24, 392–400 (2018). https://doi.org/10.1038/nm.4517
- Fan, Y. & Pedersen, O. Gut microbiota in human metabolic health and disease. Nat. Rev. Microbiol. 19, 55–71 (2021). https://doi.org/10.1038/s41579-020-0433-9
- Zmora, N., Suez, J. & Elinav, E. You are what you eat: diet, health and the gut microbiota. Nat. Rev. Gastroenterol. Hepatol. 16, 35–56 (2019). https://doi.org/10.1038/s41575-018-0061-2
- Jovel, J., Patterson, J., Wang, W., Hotte, N., O’Keefe, S., Mitchel, T. et al. Characterization of the gut microbiome using 16S or shotgun metagenomics. Front. Microbiol. 7, 459 (2016). https://doi.org/10.3389/fmicb.2016.00459
- Sczyrba, A., Hofmann, P., Belmann, P., Koslicki, D., Janssen, S., Dröge, J. et al. Critical assessment of metagenome interpretation – a benchmark of metagenomics software. Nat. Methods 14, 1063–1071 (2017). https://doi.org/10.1038/nmeth.4458
- Hugenholtz, P. & Tyson, G. W. Metagenomics. Nature 455, 481–483 (2008). https://doi.org/10.1038/455481a [Note: News article – consider replacing with peer-reviewed primary source, e.g., Quince et al. 2017 Nat. Biotechnol., doi: 10.1038/nbt.3935]
- Pribyl, A. L. et al. Critical evaluation of faecal microbiome preservation using metagenomic analysis. ISME Commun. 1, 14 (2021). https://doi.org/10.1038/s43705-021-00014-2
- Parks, D. H., Rigato, F., Vera-Wolf, P., Krause, L., Hugenholtz, P., Tyson, G. W. & Wood, D. L. A. Evaluation of the Microba Community Profiler for taxonomic profiling of metagenomic datasets from the human gut microbiome. Front. Microbiol. 12, 643682 (2021). https://doi.org/10.3389/fmicb.2021.643682
- Paone, P. & Cani, P. D. Mucus barrier, mucins and gut microbiota: the expected slimy partners? Gut 69, 2232–2243 (2020). https://doi.org/10.1136/gutjnl-2020-322260
- Cornick, S., Tawiah, A. & Chadee, K. Roles and regulation of the mucus barrier in the gut. Tissue Barriers 3, e982426 (2015). https://doi.org/10.4161/21688370.2014.982426
- Desai, M. S., Seekatz, A. M., Koropatkin, N. M., Kamada, N., Hickey, C. A., Wolter, M. et al. A dietary fiber-deprived gut microbiota degrades the colonic mucus barrier and enhances pathogen susceptibility. Cell 167, 1339–1353 (2016). https://doi.org/10.1016/j.cell.2016.10.043
- Earle, K. A., Billings, G., Sigal, M., Lichtman, J. S., Hansson, G. C., Elias, J. E. et al. Quantitative imaging of gut microbiota spatial organization. Cell Host Microbe 18, 478–488 (2015). https://doi.org/10.1016/j.chom.2015.09.002
- Zhernakova, A., Kurilshikov, A., Bonder, M. J., Tigchelaar, E. F., Schirmer, M., Vatanen, T. et al. Population-based metagenomics analysis reveals markers for gut microbiome composition and diversity. Science 352, 565–569 (2016). https://doi.org/10.1126/science.aad3369
- Thomas, A. M., Manghi, P., Asnicar, F., Pasolli, E., Armanini, F., Zolfo, M. et al. Metagenomic analysis of colorectal cancer datasets identifies cross-cohort microbial diagnostic signatures and a link with choline degradation. Nat. Med. 25, 667–678 (2019). https://doi.org/10.1038/s41591-019-0405-7
- Wirbel, J., Pyl, P. T., Karber, E., Zych, K., Kashani, A., Milanese, A. et al. Meta-analysis of fecal metagenomes reveals global microbial signatures that are specific for colorectal cancer. Nat. Med. 25, 679–689 (2019). https://doi.org/10.1038/s41591-019-0406-6